Neurocranium
Frontal
Ectocranial
- Frontal eminence (original center of ossification)
- Temporal lines (appear when you grit your teeth)
- Brow ridge
- Supraorbital margin
- Supraorbital foramen or notch (passage for vessels)
- Glabella (between the eyebrows)
- Zygomatic process of the frontal (articulates with zygomatic bone)
Endocranial
- Sagittal sulcus
- Frontal crest
- Foramen cecum
- Meningeal grooves
Inferior view
- Ethmoidal notch (location of ethmoid bone)
- Lacrima fossa (location of lacrimal gland)
- Frontal sinuses
Variations
- Metopic suture
Compared to the parietals, the minengeal impressions are fainter and the endocranial surface is more undulating.
Parietal
Angles
- Frontal angle (90 degrees)
- Sphenoidal angle
- Occiptal angle (near the occipital bone)
- Mastoid angle (near the mastoid process)
Ectocranial
- Parietal boss
- Parietal foramen (near the sagittal suture)
- Parietal striae (away from the sagittal suture)
- Temporal lines (extending from the frontal bone)
Endocranial
- Sagittal sulcus
- Sigmoid sulcus (near the mastoid angle)
- Meningeal grooves
Variations
- Bregmatic bone
- Wormian bones
Occipital
Ectocranial
- External occipital protuberence
- Highest, superior, and inferior nuchal lines
- External occipital crest (leading to the foramen magnum)
- Foramen magnum ("big hole")
- Occipital condyle (bean-shaped and articulates with C1)
- Condylar foramen (superior to the condyles)
- Hypoglossal canal (inferior to the condylar foramen)
Endocranial
- Cruciform eminence
- Cerebral fossa (triangular)
- Cerebellar fossa (quadrangular)
- Sagittal sulcus (usually swings right)
- Transverse sulcus (opp. sagittal sulcus)
- Internal occipital crest (leading to the foramen magnum)
- Jugular notch (below the foramen magnum)
- Middle meningeal grooves
Variations
- Inca bone
- Apical bone
Temporal
There are four parts of the temporal bone: squama, mastoid (right behind the ear), petrous (pyramid), and tympanic (inside).
Ectocranial
- Zygomatic process (and articulates with zygomatic bone)
- Articular eminence (right below the zygomatic process)
- Mandibular fossa (right next to the articular eminence)
- Post-glenoid process (small cone behind the mandibular fossa)
- Suprameatal crest (root of zygomatic process above the EAM)
- Supramastoid crest (extension of the suprameatal crest)
- Parietal notch (end of the crest that is level with the zygomatic process)
- Mastoid process (behind the ear)
- Mastoid notch (behind the mastoid process)
- Mastoid foramen
- External acoustic meatus (EAM)
Endocranial (posterior view)
- Internal acoustic meatus (biggest hole on the inside)
Endocranial (inferior view)
- Styloid process (pointed projection)
- Styloidmastoid foramen (under the styloid process)
- Jugular fossa (bottom-right of the styloid process)
- Cartoid canal (above the styloid process)
Splanchnocranium
Auditory Ossicles
- Stapes
- Incus
- Malleus
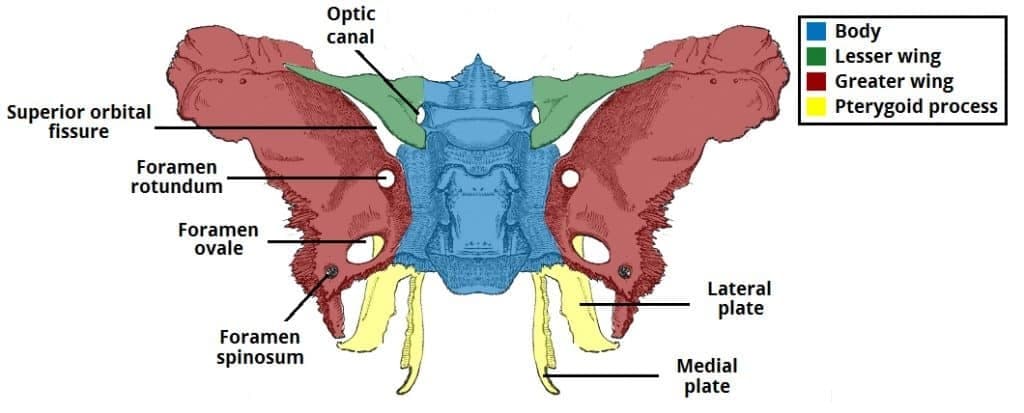
Sphenoid
The sphenoid is comprised of the body, lesser wings, greater wings, and the pterygoid process.
Posterior View
- Anterior clinoid process (hooks under the wings)
- Sella turcica (between the wings)
- Pituitary fossa (under the Sella turcica)
- Dorsum sellae (handlebars)
- Posterior clinoid process (ends of handlebars)
- Clivus (under the posterior clinoid process)
- Body (under the dorsum sellae)
Posterior View (OOROS)
- Optic canal
- Superior orbital fissures
- Foramen rotundum (round)
- Foramen ovale (oval)
- Foramen spinosum (tiny)
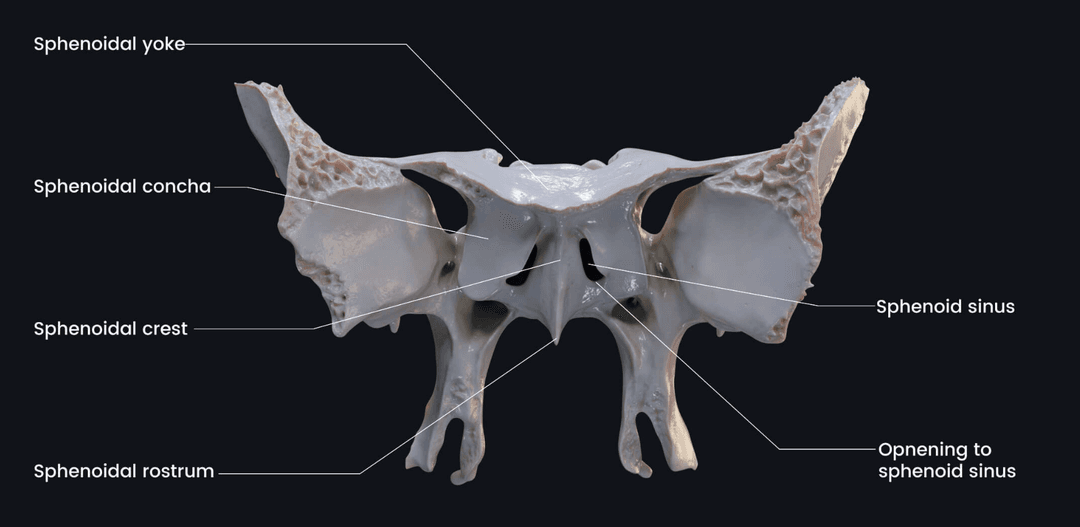
Anterior View
- Orbital surfaces
- Sphenoidal crest (middle ridge)
- Sphenoidal sinus (holes on either side of the crest)
- Sphenoidal rostrum (under the sphenoidal crest)
Anterior View (Pterygoid process)
- Medial pterygoid plate
- Pterygoid hamulus (hook on the medial pterygoid plate)
- Lateral pterygoid plate
- Pterygoid fossa (formed by the medial and lateral plates)
Ethmoid
- Crista galli (projection)
- Cribriform plate (horizontal plate)
- Perpendicular plate
- Lateral mass (labyrinth touching eye sockets)
Inferior Nasal Concha
Can see through the nasal cavity, on the sides. The maxillary process is the part that is hooked onto the side of the nasal aperture. The head is anterior and the long tail inferior. It's like a fish coming out.
Nasal
Makes up the bridge of the nose. The top that articulates with the frontal is thicker. The distal is longer than the medial.
Lacrimal
Inside of the eye socket, near the nose. The hook forms the grooves for the lacrimal glands.
Zygomatic
- Frontal process
- Orbital margin
- Temporal process
- Maxillary process
- Masseteric origin (masseter muscle attaches)
- Zygomaticofacial foramen
The anterior surface is big and flat and will have a zygomaticofacial foramen.
Maxilla
Anterior View
- Frontal process
- Zygomatic process
- Infraorbital foramen (next to zygomatic process)
- Canine jugum (from the canine root)
- Canine fossa (posterior to the canine jugum)
- Anterior nasal spine (near the nasal cavity)
- Alveolar process (houses the teeth)
- Alveolar canals (tooth sockets)
Superior view
- Anterior lacrimal crest (near lacrimals)
- Infraorbital sulcus (in the orbitals)
Posterior view
- Maxillary sinus
- Palatine process (roof of mouth)
- Incisive foramen (right behind incisors)
Canine root is distinctive to anatomically modern humans. Humans have relatively flat faces; premaxilla fuse with maxilla.
Palatine
Shaped like an L. The shorter part is the horizontal plate and should be oriented medially. The longest part is the vertical plate. The posterior has a ridge sticking out called the pyramidal process.
- Posterior nasal spine (articulates with the other palatine)
- Pyramidal process
- Greater palatine foramen (anterior)
- Lesser palatine foramen (posterior)
Vomer
Divides the nasal aperture in half. The anterior is thin and the posterior is thick.
Mandible
The mandible is divided into the body (corpus) and the ascending ramus.
External surface
- Mental eminence (chin)
- Mental foramen
- Alveolar process
- Alveolar canals
- Gonial angle
- Masseteric tuberosity (rough)
- Ascending ramus
- Mandibular condyle (more posterior than coronoid process)
- Coronoid process (more anterior than condyle)
- Condylar neck (between the condyle and the coronoid process)
- Mandibular notch
Internal surface
- Mandibular foramen
- Lingula (sticks up next to mandibular foramen)
- Pterygoid tuberosity
- Mylohyoid groove (extends from the lingula)
- Mylohyoid line (more anterior than the mylohyoid groove)
- Submandibular fossa (between the groove and the line)
- Mental spines (near the chin)
- Digastric fossa (inferior and posterior to mental spines)
The mental eminence is a distinctive feature of anatomically modern humans.
Men tend to have a more 90° gonial angle, while women tend to have a more obtuse gonial angle. Older individuals with tooth loss also tend to have a more obtuse gonial angle.
Dentition
Terms
- Mesial is toward the midline and distal is away from the midline
- Labial is toward the lips and buccal is toward the cheek
- Lingual is toward the tongue
- Interproximal is where two teeth meet
- Incisal and occlusal are biting surfaces
Humans are diphyodont, which means that they have two sets of teeth, deciduous (baby) and permanent.
Humans are also heterodonts, which means that we have different types of teeth. Incisors are used for cutting, canines for tearing, premolars for grinding, and molars for crushing.
Teeth Anatomy
Teeth have two parts (crown and root) and three layers (enamel, dentine, and pulp chamber). Connective tissue called cementum holds the teeth in place.
Teeth grow from the cusp to the cemento-enamel junction (CEJ). Roots are the last to form. Ameloblast deposit enamel at the same time as adontoblast deposit dentine.
Enamel is 96% mineral. Dentine is 70% mineral and 30% collagen. The pulp chamber is mostly nerves and blood vessels.
Adults have 32 teeth. There are four quadrants in the mouth, each with 8 teeth: 2 incisors, 1 canine, 2 premolars, and 3 molars. The third molars are the wisdom teeth. Many people have the third molar pulled out because they cause crowding.
Identifying Teeth
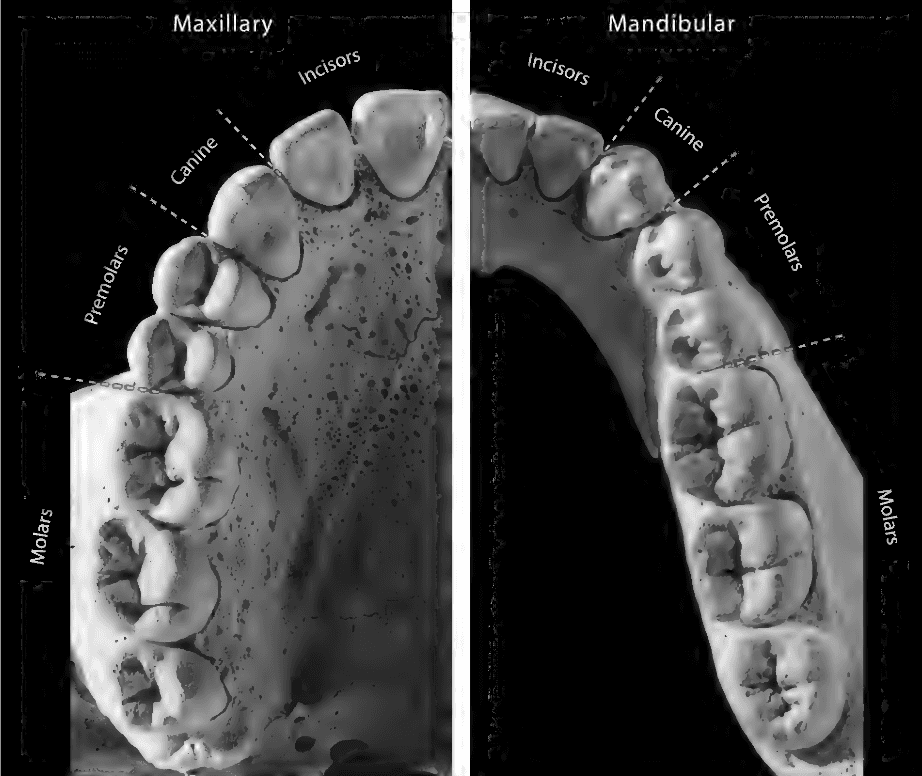
Upper incisors are generally larger, broader, and more likely to be shovel-shaped. Upper incisor roots are more circular, while lowers are more compressed. Incisors tend to be more 90 degree mesially and curved distally.
Canines tend to come to a point and tend to be wider than incisors. Upper canines are generally larger, broader, and more likely to have cingulum than the lowers.
Premolars are also called bicuspids because they have two cusps. Lowers have a larger buccal cusp than lingual cusp. Uppers sometimes have two roots (often fused). The first premolar has more asymmetric cusps than the second premolar.
Upper molars usually have 3 roots and 3-4 major cusps. Lower molars generally have 2 roots and 4-5 major cusps. The uppers tend to be square in shape while the lowers tend to be rectangular or oblong. Uppers tend to be more asymmetric around the mesiodistal axis than lowers. This is because uppers have triangular hypocone on the lingual distal end. This hypocone is largest on the first molar and smaller on the second and third.
To side the teeth, note that the roots swing distally.
Spine
Hyoid
- Body
- Greater horns
- Lesser horns
Vertebrae
General Features:
- Body
- Pedicle
- Lamina
- Spinous process (pointy bit)
- Superior articular facet
- Inferior articular facet
- Transverse process
- Vertebral foramen (where spinal cord goes through)
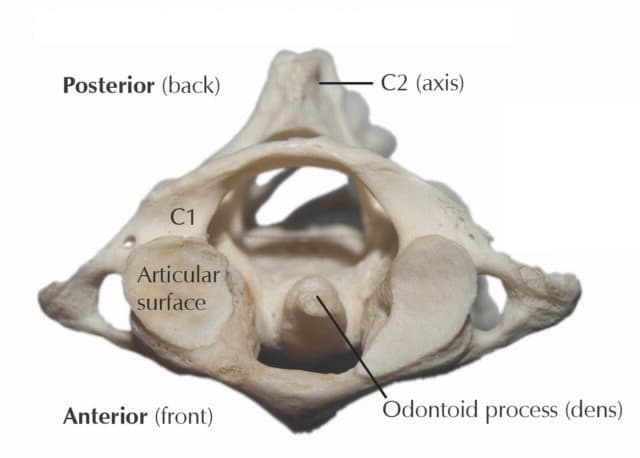
Cervical Vertebrae
Cervical vertebrae make up the bones in the neck. They can be distinguished from the other vertebrae by the presence of transverse foramina. They also may have a bifurcated spinous process and a small body. The superior and inferior articular facets are oriented in a horizontal plane.
Superior View
- Transverse foramen
- Transverse tubercle
- Facet for dens (C1, body)
- Dens (C2, protrusion on body)
- Facet for atlas (C2)
Specific vertebrae
- C1 (atlas) has no body or spinous process. In place of the body is the facet for the dens, which articulates with the dens of C2. The superior articular facets are large and concave to articulate with the occipital condyles.
- C2 (axis) and has a projection called the dens that articulates with the atlas.
Thoracic Vertebrae
The thoracic vertebrae articulates with the ribs and can be distinguished by the presense of demi-facets on the body and constal facets on the transverse process. Additonally, the superior and inferior articular facets are oriented more vertically.
Features
- Superior articular process (face posteriorly)
- Inferior articular process (face anteriorly)
- Transverse costal facet (on the transverse process, articulates with rib)
- Superior costal demi-facet (on the body, articulates with rib)
- Inferior costal demi-facet (on the body, articulates with rib)
Specific vertebrae:
- T10 has a single rib facet and a transverse costal facet.
- T11 has a single rib facet and no transverse costal process.
- T12 has a signle rib facet and no transverse costal process. However, it has inferior articular facets that are oriented like lumbar vertebrae.
Lumbar Vertebrae
Lumbar vertebrae have large bodies and short, blunt spinous processes. They can be distinguished by the lack of transverse foramina and costal facets.
- Superior articular process
- Inferior articular process
- Mammilary process (knob on the superior articular process)
Pelvic Girdle
Os Coxae
The os coxae makes up the pelvis. It is made up of three bones that fuse together in adulthood:
- Ilium (large flaring part of the hips)
- Ischium (where you sit on)
- Pubis (where the pelvis meets in the front)
It also has two landmarks:
- Obturator foramen (big hole covered by membrane)
- Acetabulum (hip sockets)
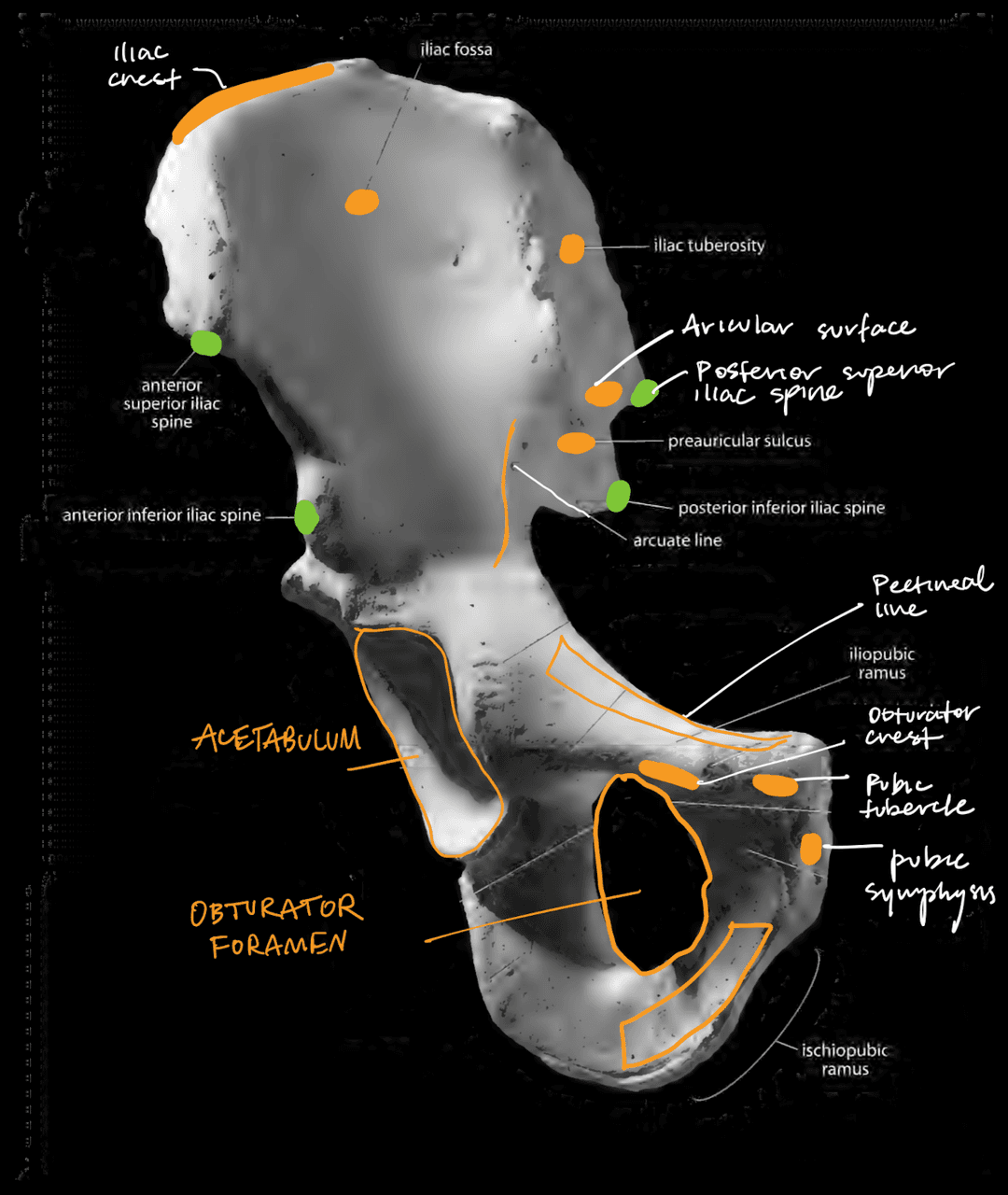
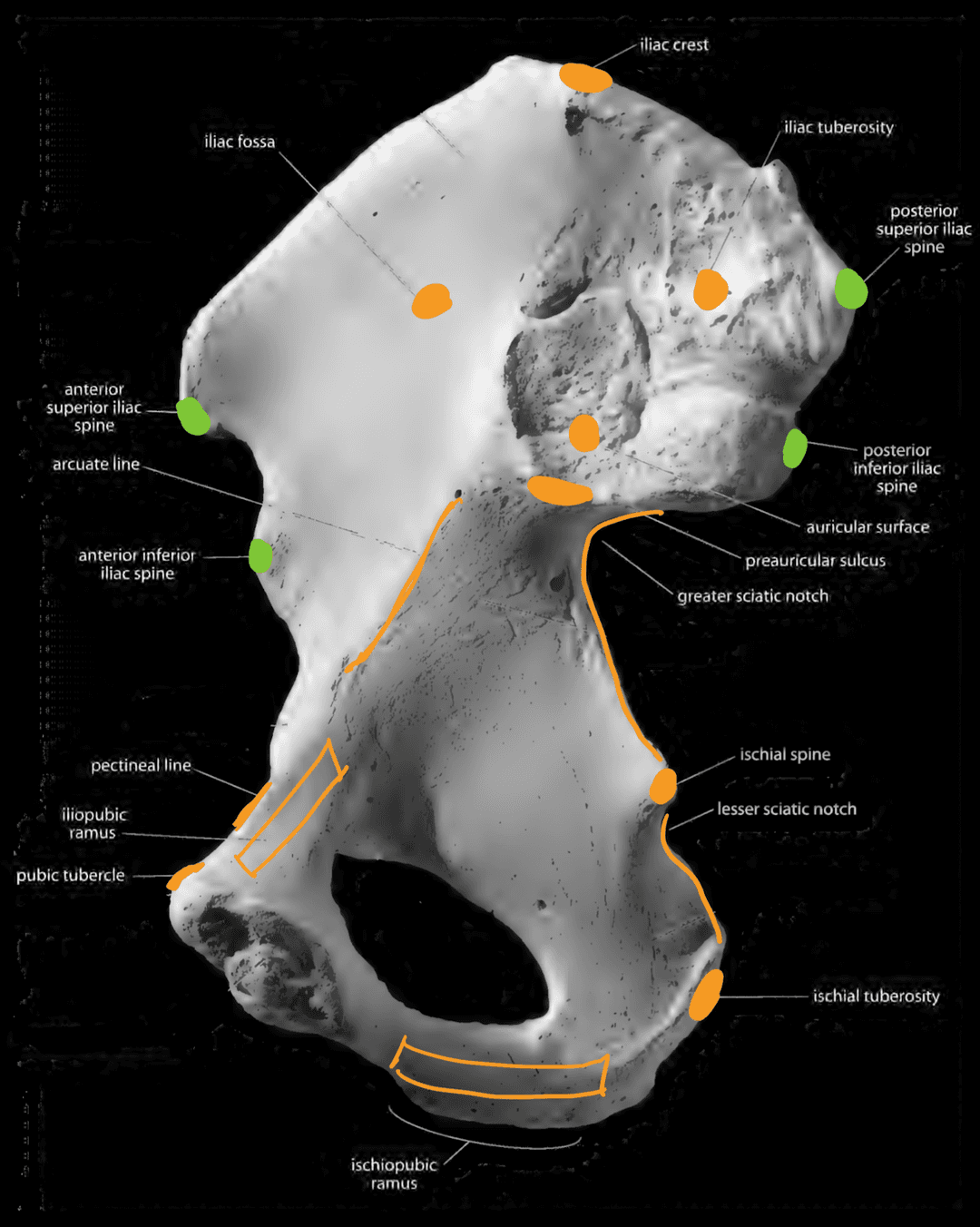
Illium and Ischium (Anterior View)
- Iliac crest (top of the ilium)
- Iliac fossa (bowl)
- Iliac tuberosity (back of ilium, behind the auricular surface)
- Auricular surface (immovable joint where the sacrum articulates with the ilium)
- Preauricular sulcus (sulcus below the auricular surface)
- Arcuate line (coming from base of iliac fossa)
- Iliac spines (anterior-superior, anterior-inferior, posterior-superior, posterior-inferior)
- Greater sciatic notch
- Ischial spine (divides the sciatic notches)
- Lesser sciatic notch
- Ischial tuberosity
Pubis (Anterior View)
- Illiopubic ramus
- Pubic tubercle
- Ischiopubic ramus
- Obturator crest (anterior)
- Pectineal line (posterior)
- Pubic symphysis (where the pubic bones articulate)
Acetabulum
- Lunate surface
- Acetabular fossa
Posterior View
- Anterior gluteal line (starts at the top of the iliac crest)
- Posterior gluteal line (starts at the start of the iliac crest)
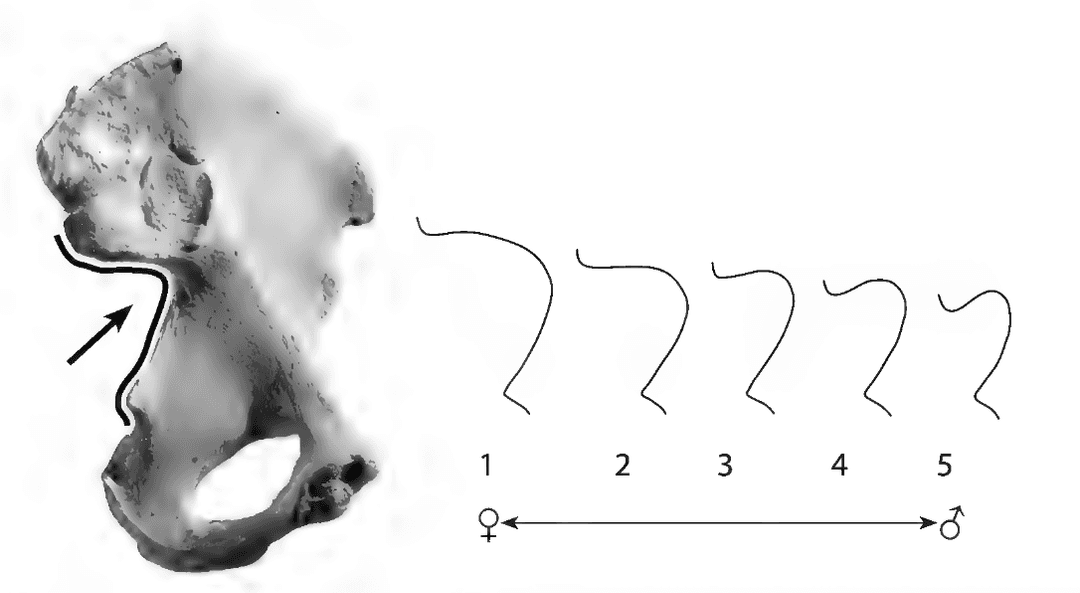
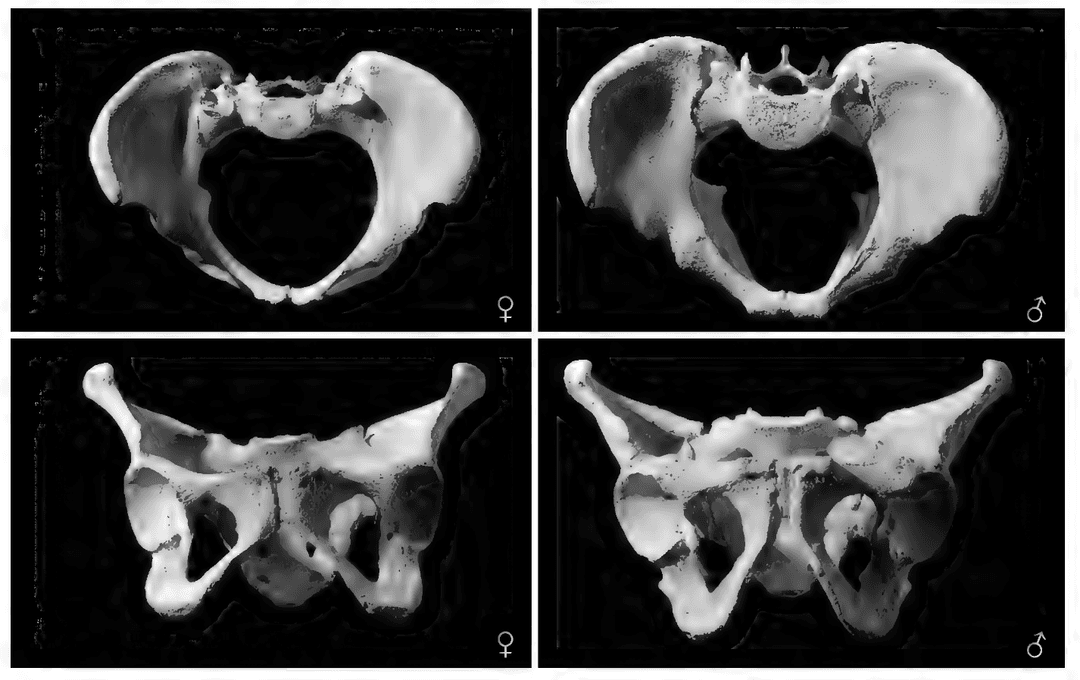
Males tend to have a smaller greater sciatic notch. Females tend to have a preauricular sulcus.
Sacrum
The sacrum is made up of five fused vertebrae. It articulates with the ilium at the auricular surface and with the coccyx at the sacral hiatus.
Anterior View
- Sacral plateau (top of sacrum)
- Sacral promontory (ridge on plateau)
- Anterior sacral foramina (holes)
- Transverse ridges (bridge the holes)
Lateral View
- Ala (wings on either side)
- Auricular surface (articulates with the ilium)
Posterior View
- Sacral canal (houses spinal cord)
- Superior articular process (juts out)
- Superior articular facet (similar to the vertebrae)
- Dorsal wall (back surface)
- Median sacral crest (midline ridge)
- Lateral sacral crest (lateral to the holes)
- Posterior sacral foramina (holes)
- Sacral hiatus (opening at the of sacral canal)
- Sacral cornu (horn-like projections at apex)
The coccyx is a triangular bone at the base of the spine consisting of multiple fused vertebrae.
Pectoral Girdle
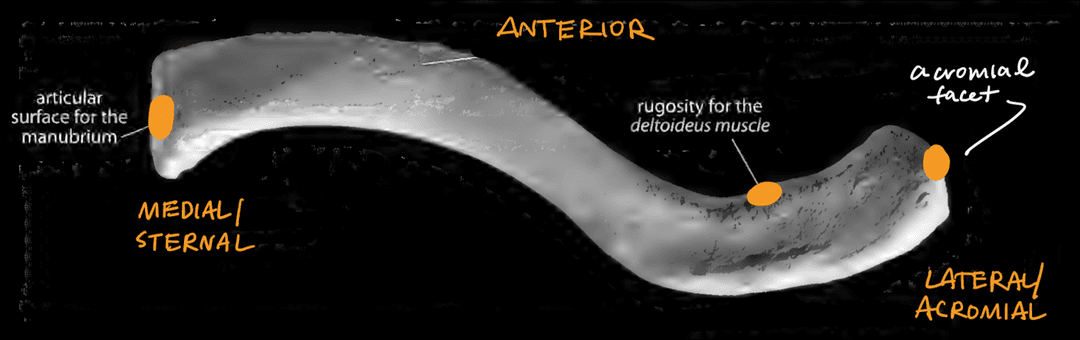
Clavicle
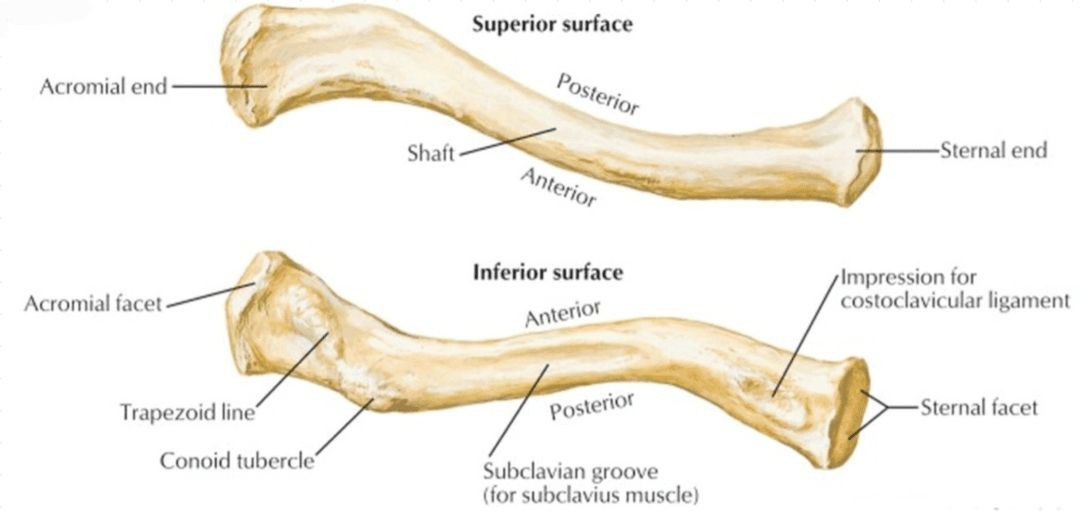
The clavicle, also known as the collabone, serves as a strut between the scapula and the sternum.

The rounder and thicker end is medial and articulates with the sternum. The flatter end is lateral and articulates with the scapula. The medial end tends to points backward and the lateral end tends to point forward. The superior side is smooth and the inferior side is rough. The inferior side also has a sulcus.
Superior View
- Articular surface for the manubrium (articulates with the sternum)
- Rugosities for the deltoid muscle
- Arcomial facet
Inferior View
- Costoclavicular impression (connects with the first rib)
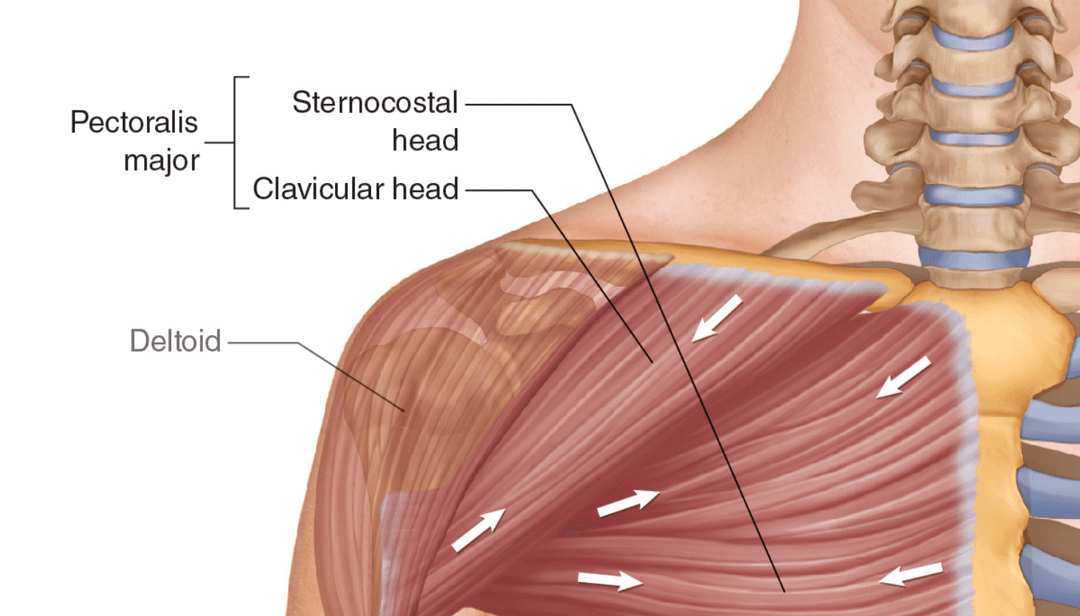
- Rugosities for the pectoralis major muscle
- Subclavian groove
- Conoid tubercle
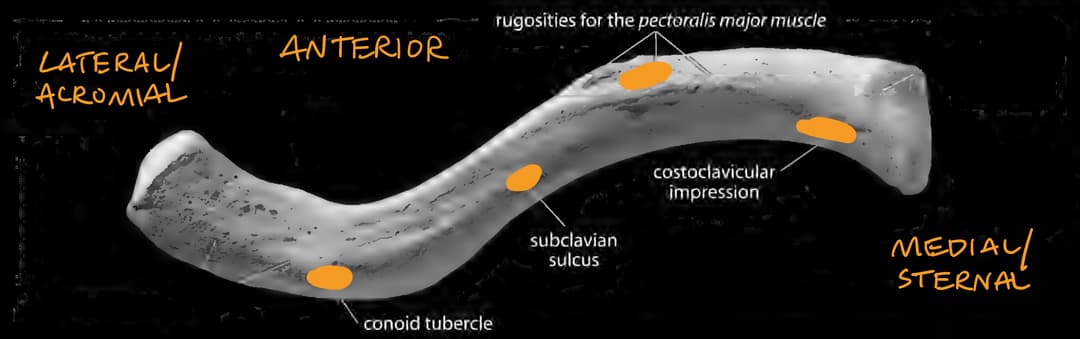
Here are some clearer images of the costoclavicular impression, subclavian groove, and conoid tubercle:
Note that the deltoid muscle attaches to the lateral, superior side of the clavicle, while the pectoralis major muscle attaches to the medial, inferior side near the pecs. The subclavian groove is where the subclavius muscle attaches.
The clavicle is the first bone to start ossification and last bone to finish ossification.
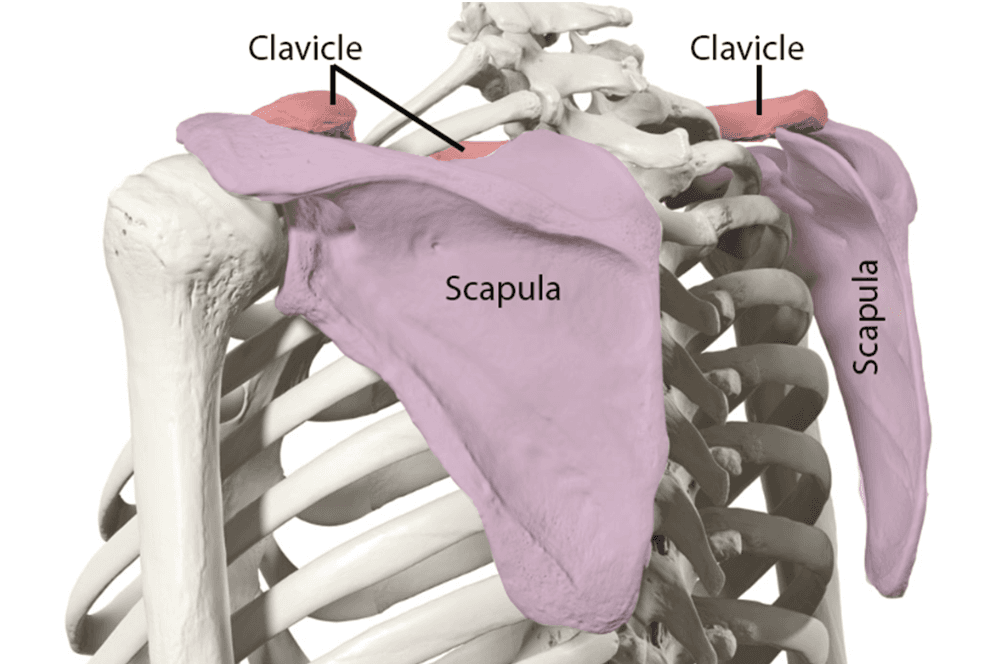
Scapula
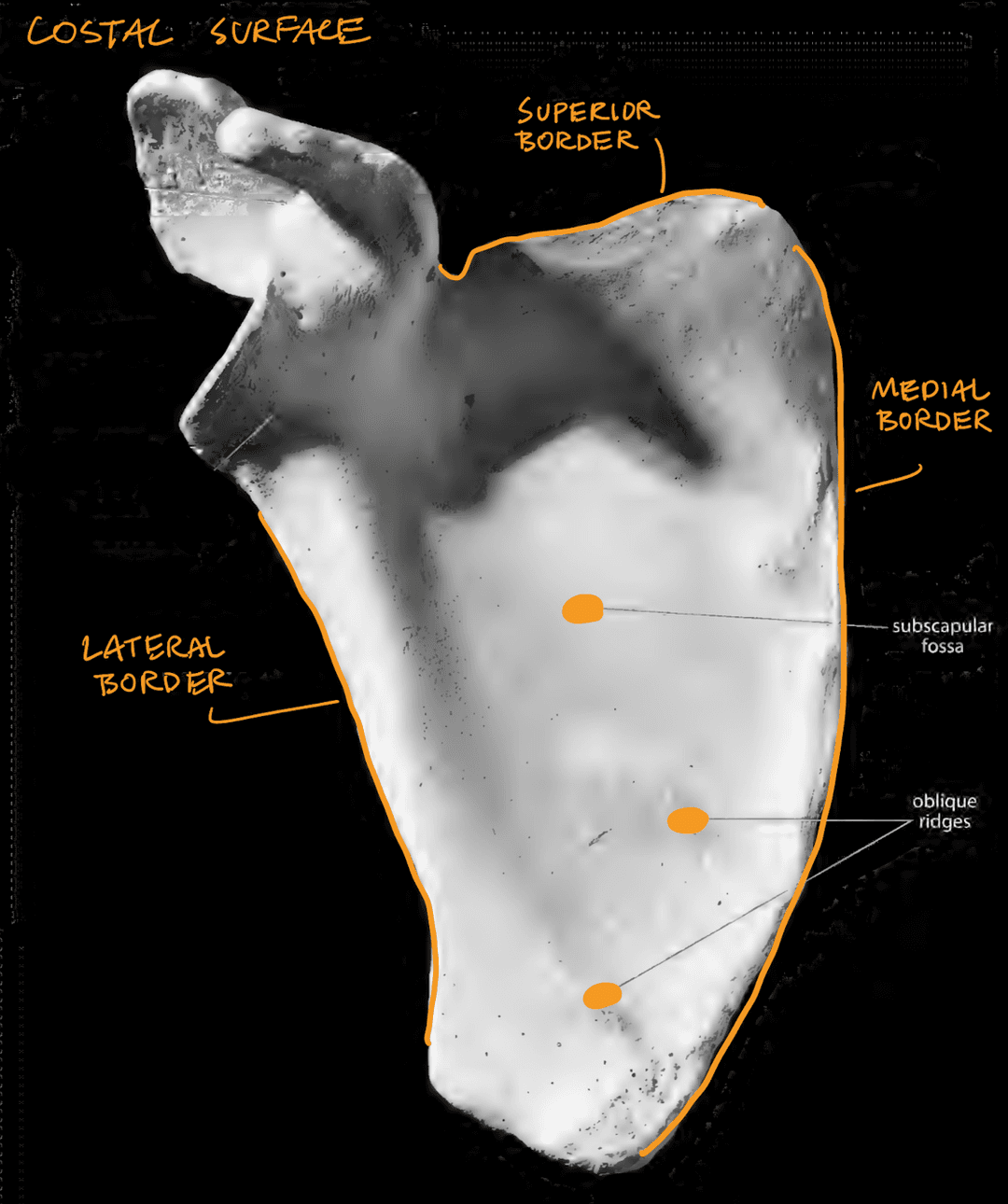
The scapula, also known as the shoulder blade, is a flat bone that connects the humerus with the clavicle. It has two surfaces (dorsal and costal) and three borders (superior, medial, and lateral).
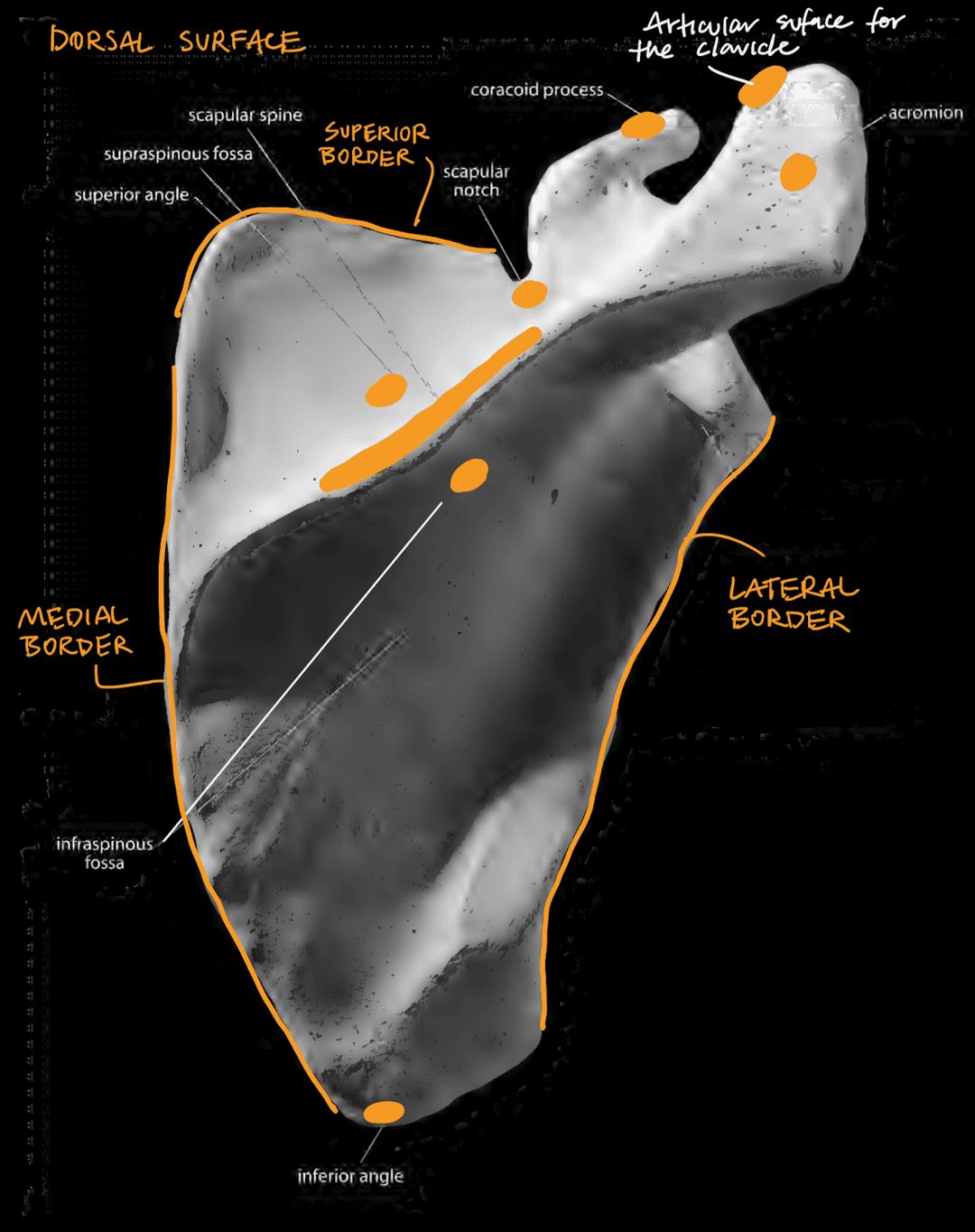
General
- Dorsal surface (has acromion)
- Costal surface (facing ribs, does not have acromion)
- Superior border (shortest side of the triangle)
- Medial border (facing toward the vertebrae)
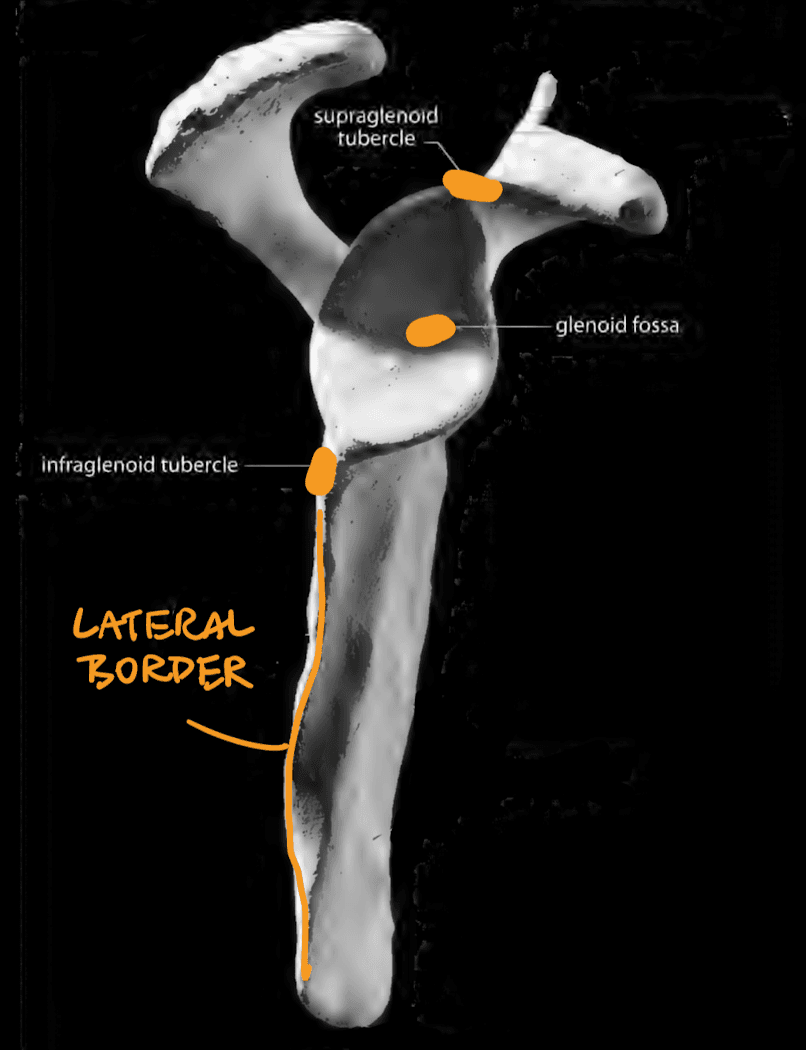
- Lateral border (toward the arms)
Dorsal Surface
- Acromiom (articulates with the clavicle)
- Articular facet for the clavicle (articulates with the clavicle)
- Coracoid process (smaller projection, sticks anteriorly)
- Scapular notch (near the coracoid process)
- Scapular spine (base of the acronium)
- Supraspinous fossa
- Infraspinous fossa
- Inferior angle (bottom of the triangle)
Costal Surface
- Subscapular fossa (large area)
- Oblique ridges (bottom third of scapula)
Lateral View
- Glenoid fossa (flat area that articulates with the humerus)
- Supraglenoid tubercle (apex of the glenoid fossa)
- Infraglenoid tubercle (bottom of the glenoid fossa)
Thorax
Sternum
The sternum is divided into the manubrium and the body, which may fuse later.
To orient the sternum, note that there are demifacets where the manubrium and the sternum meet. There is also a huge gap between costal notches 2 and 3.
Features
- Jugular notch (top of sternum)
- Clavicular notch (articulates with the clavicle)
- Costal notch 1
- Costal notch 2 (where the manubrium and body meet)
- Costal notches 3-7 (articulates)
- Xiphoid process (bottom of sternum)
Variations
- Sternal foramen
- Cleft sternum
Note that the sternum articulates with the ribs (costal cartilage) at the costal notches. The first rib articulates with the manubrium, while ribs 2-7 articulate with the body. Ribs 8-10 articulate with the costal cartilages of the ribs above them.
Ribs
R1-R7 are called with the true ribs because they articulate directly with the sternum. R8-R10 are called the false ribs because they articulate with sternum via other rib cartilate. R11 and R12 are called floating ribs because they do not articulate with the sternum at all.
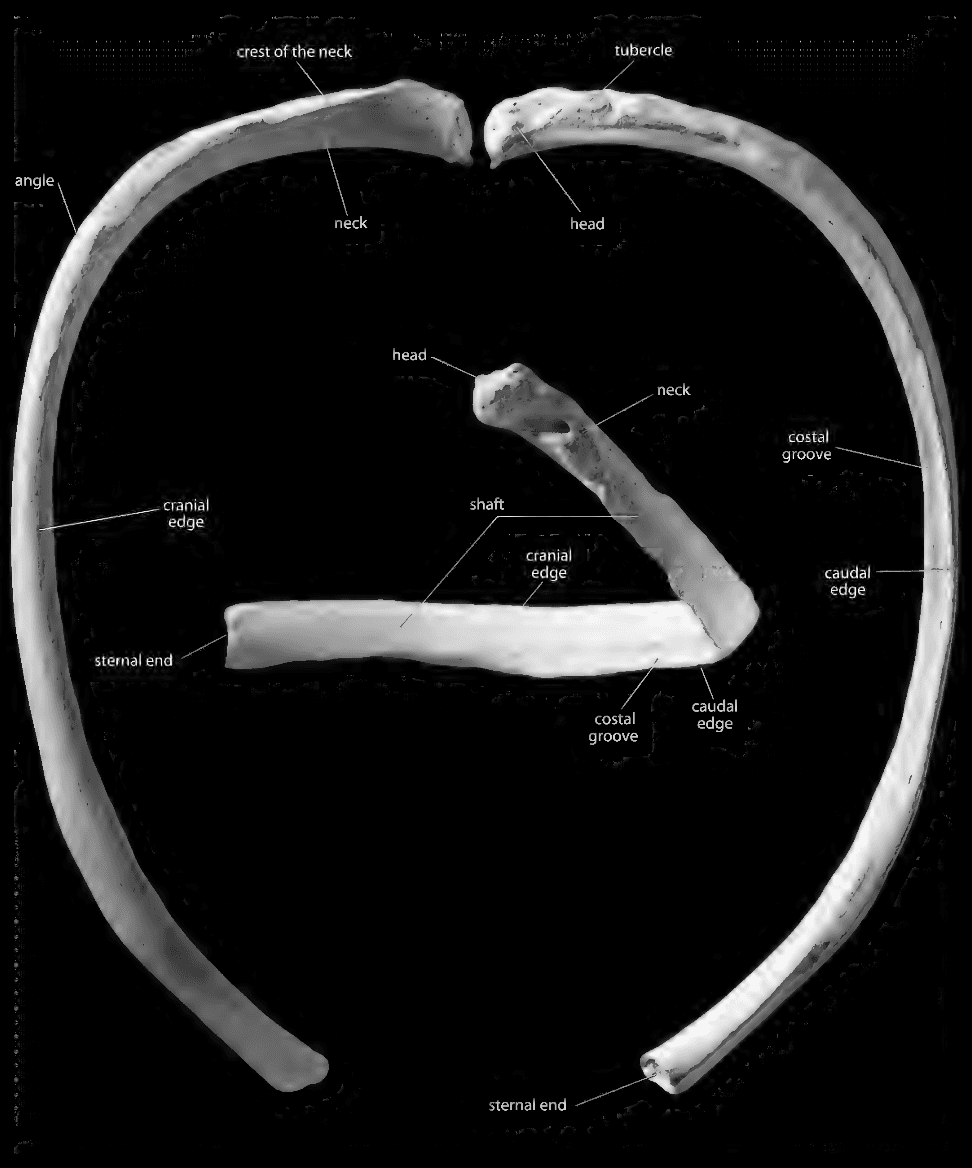
The vertebral end has a head that articulates with the vertebrae, while the sternal end is flat and blunt. The rib sits between two vertebrae, so the head is often bifurcated. The caudal edge is on the inferior side of the rib.
R1-R10
- Head (round and articulates with the inferior and superior costal demi-facets)
- Neck (between head and tubercle)
- Tubercle (inferior, articulates with transverse process of vertebrae)
- Angle (where the rib starts to curve)
- Shaft (body of the rib)
- Costal groove (inferior, runs from tubercle to angle)
- Caudal edge (inferior)
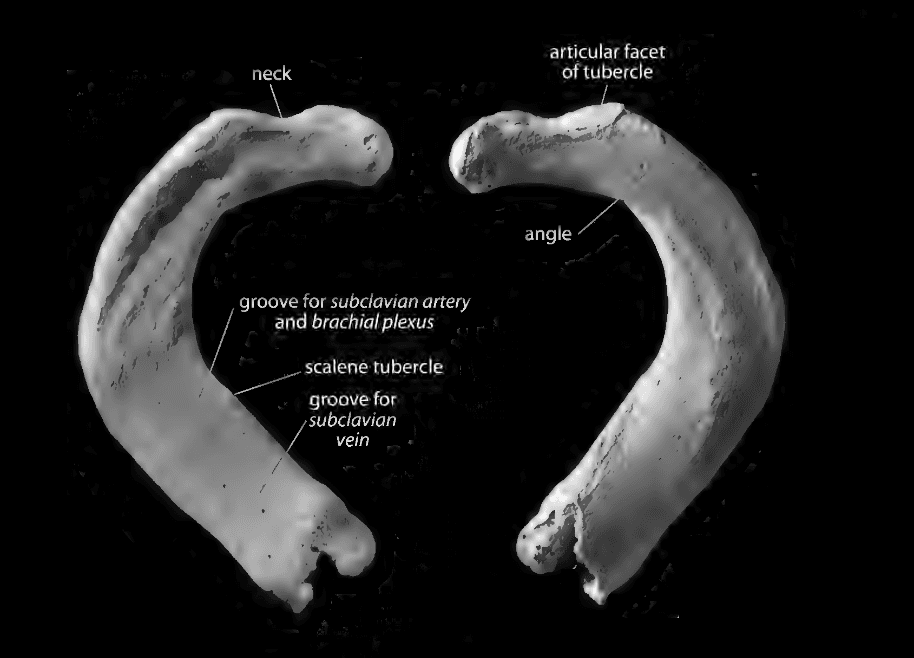
The first ribs are flat and have all the features of the other ribs. The head has only one facet. To side it, find the grooves; they should be superior.
R1
- Scalene tubercle (between the grooves)
- Groove for subclavian artery (superior, vertebral end)
- Groove for subclavian vein (superior, sternal end)
R10 is just like R1-R9, but it only has one facet. It is fairly flat, so it might be difficult to identify the caudal edge.
R11 and R12 have a single facet on the head and do not have a tubercle. R11 has a slight angle to it, whereas R12 does not. Hold it by the head straight up and check the angle. To side it, orient it so that, from the anterior perspective, you can see the medial face.
Arms
Humerus
The proximal end is the ball-and-socket, and the distal end has two round areas which articulate with the ulna and the radius.
To side the whole humerus, note that the medial epicondyle (knob) should be medial and the olecranon fossa (large depression) should be posterior. Additionally, the humeral head should lean in the direction of the shoulder.
If you just have a shaft end, you may be able to side it using the nutrient foramen. They are all angled: "flees the knees, flows to the elbows."
Proximal End
- Humeral head
- Greater tubercle (anterior, lateral)
- Lesser tubercle (anterior, medial)
- Crest of the lesser tubercle
- Crest of the greater tubercle
- Intertubercular groove
- Anatomical neck
- Surgical neck
Shaft
- Deltoid tuberosity (starts laterally turns medially)
- Nutrient foramen (midshaft, anterior)
Distal End
- Olecranon fossa
- Trochlea (articulates with the ulna)
- Capitulum (articulates with radius)
- Coronoid fossa (anterior, above trochlea)
- Radial fossa (anterior, above capitulum)
- Medial epicondyle (medial to articular surface)
- Lateral epicondyle (lateral to articular surface)
- Medial supracondylar crest
- Lateral supracondylar crest
Ulna
In standard anatomical position, the ulna is medial to the radius. It is thicker proximally than medially.
To identify the ulna, note that it has an olecranon (u-shaped hook) which locks into the back of the humerus. To side it, note that the radial notch is lateral.
Proximal end
- Olecranon (U-shaped hook that sits in olecranon fossa)
- Trochlear notch (under olecranon)
- Coronoid process (horn that ends the trochlear notch)
- Radial notch (lateral)
- Supinator crest (anterior, comes off the radial notch)
- Ulnar tuberosity (anterior, under the coronoid process)
Shaft
- Interosseous crest (sharpest border, lateral)
- Nutrient foramen (near the proximal 1/3)
Distal end
- Ulnar head
- Styloid process (juts out)
- Articular circumference (what the radius flips around on)
- Extensor carpi ulnaris groove (lateral to the styloid process)
Radius
In standard anatomical position, radius is lateral to the ulna. It is thinner proximally than distally. It is less triangular than the ulna. The proximal end of the radius looks similar to the distal end of the ulna, but it does not have a styloid.
To side it, notice that on the distal end, the smooth surface is anterior and the the side with bumps and grooves is posterior. On the distal end, the radial styloid process should be lateral and the ulnar notch should be medial.
Proximal end
- Radial head
- Radial neck (distance between head and radial tuberosity)
- Radial tuberosity (medial and anterior)
Shaft
- Interosseus crest (medial toward the ulna)
- Nutrient foramen
- Anterior oblique line (extend from the tuberosity)
- Posterior oblique line (extend from the tuberosity)
Distal end
- Styloid process (lateral)
- Ulnar notch (posterior, medial)
- Dorsal tubercle (posterior, largest bump)
- Articular facet for lunate (closer to the ulnar notch)
- Articular facet for scaphoid (closer to the styloid process)
Hands
Each hand has 27 bones, for a total of 54 bones. That's around 1/4 of all bones in the human skeleton.
There are three parts of the hand:
- Carpals (wrist)
- Metacarpals (palm)
- Phalanges (fingers)
Sesamoid bones can develop within tendons on the hands.
Carpals
The carpus has 8 bones in 2 rows.
Proximal row
- Scaphoid (deep facet)
- Lunate (crescent moon)
- Triquetral (triangular wedge)
- Pisiform (pebble, one facet for the triquetral)
Distal row
- Trapezium (many facets, one groove)
- Trapezoid (boot)
- Capitate (big round head)
- Hamate (hamulus hook)
To side the scaphoid, put your thumb on the largest groove and your pointer finger on the smooth surface. The tubercle swings toward the side of the bone. You can also hold it with the head (the concave surface) facing you, with the tuberosity upward. The side of the bone will be the side the tuberosity is on the body.
To side the lunate, put the groove on your thumb, like it's a finger nailextension. Then take a look at which side the facet is leaning.
To side the triquetral, hold the flatest surface with your pointer finger and orient it on top. Then look at the facet for the hammate (largest facet). The facet for the pisiform will be on the side of the bone it is.
To side the pisiform, orient the bulk on top and take a look at the facet. The pisiform groove will be on the side it's on.
To side the trapezium, hold it so you are facing the saddle, with the facet posterior to you. Orient it so that the ridge is on top. The ridge will be on the side it's on.
To side the trapezoid, orient it so that the zipper of the boot faces you. The toe of the boot points to the side.
To side the capitate, look for the flat articular surface on the helmet. The flat articular surface will be on the side of the bone it's from.
To side the hamate, orient the hamate so that it is waving toward you. The hamate will be on the side of the bone it's from.
Hand phalanges
There are three types of phalanges:
- Proximal
- Intermediate
- Distal
The palmar aspect of the hand phalanges is flat, while the dorsal aspect is rounded. Feet phalanges are rounded on both aspects.
Proximal phalanges have a large rounded single facet for the metacarpal. The intermediate and distal phalanges have a double facet for the phalangeal trochlea. The distal phalanges have a roughened edge on the palmar aspect for the fingertips.
Metacarpals
Metacarpal 1 has a saddle-shaped sellar joint. The palmar side has two knobs on the distal end. To side it, it swings up higher laterally (i.e. on the side it's from).
Metacarpal 2 has a "B" shaped facet that articulates with metacarpal 3. Thus, the longer side is medial. On the distal end, the palmar view is rounder than the dorsal view.
Metacarpal 3 is the only one with a styloid process, which faces metacarpal 2. It also has two facets facing metacarpal 4. On the distal end, the palmar view is rounder than the dorsal view.
Metacarpal 4 has two small facets facing metacarpal 3 and one large facet facing metacarpal 5.
Metacarpal 5 only has one facet facing metacarpal 4.
Legs
Femur
The posterior aspect of the femur has more muscle attachments than the anterior aspect.
To side a proximal femur, note that the fovea capitis faces inferior, and the anterior neck is flatter than the posterior neck. The posterior neck has a bit of a bump. To side a distal femur, note that the straight short condyle is lateral and the longer curved one is medial. If you put the fermur up on a table, it will lean laterally.
- Femoral head (rounded part that articulates with acetabulum)
- Fovea capitis (depression near center of head, faces inferior)
- Femoral neck
- Greater trochanter (lateral, blunt prominence)
- Lesser trochanter (medial, posterior prominence)
- Trochanteric fossa (posterior, above greater trochanter)
- Intertrochanteric crest (posterior, above greater trochanter)
- Intertrochanteric line (anterior)
- Spiral line (starts medial and curves lateral, intertrochanteric line to linea aspera)
- Pectineal line (between the spiral line and gluteal tuberosity)
- Gluteal tuberosity (greater trochanter to linea aspera)
- Linea aspera (continues down and splits into two lines)
- Medial supracondylar line (medial split of linea aspera)
- Lateral supracondylar line (lateral split of linea aspera)
- Popliteal surface (surface between the supracondylar lines)
- Medial epicondyle (longer and curved)
- Lateral epicondyle (shorter and straight)
- Patellar surface (anterior, between two condyles)
- Intercondylar fossa (posterior, between two condyles)
- Nutrient foramen (adjacent to the linear aspera)
Patella
The rough side of the patella is anterior and the smooth end is posterior and articulates with the femur. The apex of the patella faces downward.
To side the patella, put it on a flat surface with the posterior surface down and the apex pointing away from you. The patella will fall on the side it is from.
Tibia
The tibia is always medial to the fibula.
The tibial tuberosity is anterior. To side a proximal tibia, note that the superior fibular articular facet is lateral, as is the interosseous crest. To side a distal tibia, note that the medial malleolus is medial.
- Tibial plateau
- Medial condyle (larger)
- Lateral condyle (smaller)
- Intercondylar eminence (raised area between condyles)
- Medial intercondylar tubercle (on the eminence)
- Lateral intercondylar tubercle (one the eminence)
- Superior fibular articular surface (posterior and lateral, articulates with the fibula)
- Tibial tuberosity (anterior, where you feel your knee)
- Popliteal surface (posterior to the tibial tuberosity)
- Anterior crest
- Popliteal line (starts from the superior fibular articular surface and spirals medially)
- Nutrient foramen (posterior, on the popliteal line)
- Interosseous crest (posterior)
- Medial malleolus (inside of ankle)
- Fibular notch (opposite the medial malleolus)
- Talar facet (articulates with talus)
- Anterior colliculus (most inferior aspect)
- Intercollicular groove (between the collicula)
- Posterior colliculus
Fibula
The fibula is always lateral to the tibia.
The proximal end is chunkier and the distal end is more flattened. To side the proximal fibula, face the anterior side. The articular surface will lean toward the side it's from.To side the distal fibula, note that the lateral malleolus is lateral. To side the shaft, put your thumbs on either side of the nutrient foramen. The hand touching the anterior border will be opposite of the side the fibula is from.
- Fibular head
- Styloid process
- Proximal fibular articular surface
- Fibular neck
- Anterior border (sharpest border)
- Posterior border
- Posteromedial border (only present proximally)
- Interosseous crest
- Nutrient foramen
- Lateral malleolus
- Malleolar articular surface
- Malleolar fossa
Foot
No longer a grasping foot; adapted for bipedalism. Transverse and longitudinal arch absorbs shock.
Terminology:
- Dorsal is top of foot
- Plantar is sole of foot
- Proximal is toward the tibia
- Distal is toward the toe
Each foot has 26 bones, divided into tarsals (7), metatarsals (5), and phalanges (14).
Tarsals
Proximal row
- Talus (second largest bone, superior to calcaneus)
- Calcaneus (largest bone, ankle)
Intermediate row
- Navicular (snail)
Distal row:
- Cuboid
- Medial cuneiform (eagle)
- Intermediate cuneiform
- Lateral cuneiform
The talus is the second-largest bone in the foot. It has a massive articular surface that articulates with the tibia, and distal head pointing toward the toes. The convex surface is superior and concave surface is inferior.
If you look at the bone superiorly, with the head pointed away from you, the head will always fall on the side of the big toe. Additionally, the lateral process, which articulates with the fibula, will be on the side the bone is on.
Features:
- Head
- Neck
- Sulcus tali (inferior)
- Body
- Lateral process (lateral to the superior articular facet)
The calcaneus is the largest bone in the foot, and forms most of the ankle. To side it, note that the posterior talar facet is the largest articular surface and points superiorly. The medial talar facet next to it points medially.
Features:
- Calcaneal tuberosity (near the heel)
- Sustentaculum tali (under medial talar facet)
- Sustentaculum sulcus (under medial talar facet)
- Peroneal tubercle (on the lateral aspect)
The navicular sites on the head of the talus. It has one big concave articular facet. To side it, look at the superior surface and orient the tubercle so that it is facing downward. The tubercle will be on the side that it is from.
Features:
- Tubercle
The cuboid sits on the lateral side of the foot, above the calcaneus. It is the third largest bone in the foot. It has a projecting, pointed articular surface. To side it, note that the largest facet is the facet for the calcaneus, and the opposite side is the two facets for MT4 and MT5. Orient so that you are lateral between the two facets, looking at the facet for the lateral cuneiform. Make sure the facet for the lateral cuineform is on the bottom of the body. The bone is on the side that the facet for MT4 and MT5 is.
The medial cuneiform is the fourth largeset bone in the foot and is right below MT 1. The beak of the eagle points to the side of the bone it's from.
To side the intermediate cuneiform, take a look at the convex gun. It will be pointing in the direction it is from.
The lateral cuneiform has a large circular facet for the cuboid. Look at the body with a facet on it; orient it so that the facet is on the bottom. The facet should be on the side that the bone is from.
Metatarsals
The plantar surface has a big arch; the dorsal surface is flat. On the superior aspect, they are widest on the top and narrow on the bottom.
The first metatarsal is the largest metatarsal. The second metatarsal has 2 facets medially and 1 facet laterally. The third metatarsal has 1 facet medially and 2 facets laterally. The fourth metatarsal has 1 facet laterally and 1 facet medially. The fifth metatarsal has a styloid process and only 1 facet medially.
To side the second to fifth metatarsals, look at the dorsal side (flat side) and set it on the table. It will lean opposite the side it is from.
Foot Phalanges
There are three types of foot phalanges:
- Proximal
- Distal
- Intermediate
Proximal phalanges have one facet, while intermediate and distal phalanges have two facets. Distal phalanges are also roughened on the palmar surface. The head of the first metatarsal tend to have two sesamoid bones.
Hand phalanges have shafts with flattened palmar surfaces. Foot phalanges have a circular cross section. Toe phalanges are smaller, except for the first digit.
Bone Biology
Composition and Function
Bone is 70-80% mineral (hydroxyapatite) and 20-30% organic (collagen). The collagen prevents the bone from becoming brittle.
Bone acts as both an organ and a tissue. As an organ, bone protects soft tissues; anchors muscles, tendons, and ligaments; and acts as levers for movement. As a tissue, bone produces blood cells and acts as a reservoir of nutrients (calcium, fat).
Human bones vary widely. There are four main types of variation: ontogeny (development), sexual dimorphism, geography (population), and individual.
The human skeleton is constantly remodeling in response to stress. Wolff's Law states that bone is deposited where needed and resorbed where not needed.
Musculoskeletal System
Joints are the structure between bones. There are three main types of joints:
- Synovial joints are freely movable. They include ball-and-socket joints (hip), hinge joints (elbow, knee), saddle-shaped joints (thumb), and planar joints (wrist, foot arch).
- Cartilaginous joints are made of cartilage and allow limited movement. One example are growth plates, which temporarily connect growth centers in a single bone.
- Fibrous joints are immovable (cranial sutures).
Cartilage is a flexible connective tissue found in joints. It is composed mostly of collagen.
Ligaments connect bone to bone to stabilize joints. Tendons connect muscle to bone to facilitate movement. Both ligaments and tendons are connective tissue made of collagen.
Anatomy
Bones can be categorized based on their shape
- Long bones include the arms and legs
- Short bones include metacarpals (hands), phalanges (fingers), and clavicles (collarbones)
- Flat bones include the cranial vault, scapulae, sternum (breastbone), ribs, and innominate (hipbone)
- Irregular bones include carpals (wrists), tarsals (ankles), and vertebrae
- Sesamoid bones are small, round bones embedded in tendons, like the patella (kneecap)
Bones can also be categorized based on their internal structure
- Compact bone is hard and makes up the outer layer of bones
- Spongy (cancellous) bone is porous and makes up the inner layer of bones
- Subchondral bone is covered by cartilage in joints
The long bone has several areas:
- The epiphysis (end of bone) develops from secondary ossification centers
- The diaphysis (shaft) develops from the primary ossification center
- The metaphysis is the area between the epiphysis and diaphysis where growth plates are located
- The medullary cavity is the hollow center of the diaphysis that contains bone marrow
The periosteum is a membrane that covers the outer surface of bones. It contains blood vessels, nerves, and cells that help with bone growth and repair.
Histology
Histology is the study of tissues at the microscopic level.
The Haversian system (osteon) is the basic structural unit of compact bone. It consists of concentric layers (lamellae) of bone tissue surrounding a central canal (Haversian canal) that contains blood vessels and nerves. Within each lamella, there are small cavities called lacunae that house bone cells (osteocytes).
There are three primary types of bone cells:
- Osteoblasts lay new bones and become osteocytes
- Osteocytes live in lacunae and maintain bone tissue
- Osteoclasts resorb bone
Ossification
There are two types of ossification (bone formation):
- In intramembranous ossification, mesenchymal tissue is directly converted into bone.
- In endochondral ossification, a cartilage model is first formed and then replaced by bone. This process is responsible for the formation of most bones in the body.
Primary centers of ossification appear during fetal development and form the diaphysis. Secondary centers of ossification appear after birth and form the epiphyses.
The process of bone growth occurs through two main mechanisms:
- The bone grows in length at the growth plates located in the metaphysis.
- The bone grows in width with the help of nutrient foramen, or openings in the bone that allow blood vessels to enter.
As a result of ossification, a child has around 270 bones, while an adult only has around 206 bones,
Non-Human Bone
Human bones tend to be more dense and have less trabeculae in the ends than non-human bones.
Burial Excavation
Steps:
- Pedestaling (removing dirt)
- Documentation
- Lifting (packaging the bones individually)
- Washing
- Soft tissue removal (with dermestid beetles)
- Reassembly (with Arcyloid B-72)
- Accession (labeling)
- Inventory
Acryloid B-72 is inorganic, won't degrade over time, and is dissolvable in acetone.
Afterward burial excavation, one can do sex estimation, age estimation, and checking for pathologies.
Sex Estimation
The best way to perform sex estimation is to look at the os coxae, skull and then metrics. However, no method of sex estimation is perfect.
Sex Estimation with the Os Coxae
| Feature | Female | Male |
|---|---|---|
| Greater sciatic notch | Rainbow | Hook |
| Subpubic angle | Concave | Less concave |
| Ventral arc | Pointer | Less pointy |
| Ischiopubic ramus | Pinched | Less pinched |
| Prearicular sulcus | More pronounced | Less pronounced |
Sex Estimation with the Skull
| Feature | Female | Male |
|---|---|---|
| Mastoid process | Shorter | Longer |
| Supraorbital margin | Sharper | Chunkier |
| External occiptal protuberence | Less hooked | More hooked |
| Glabella | Less pronounced | More pronounced |
| Brow ridge | Less pronounced | More pronounced |
| Mental eminence | Less pinched | More pinched |
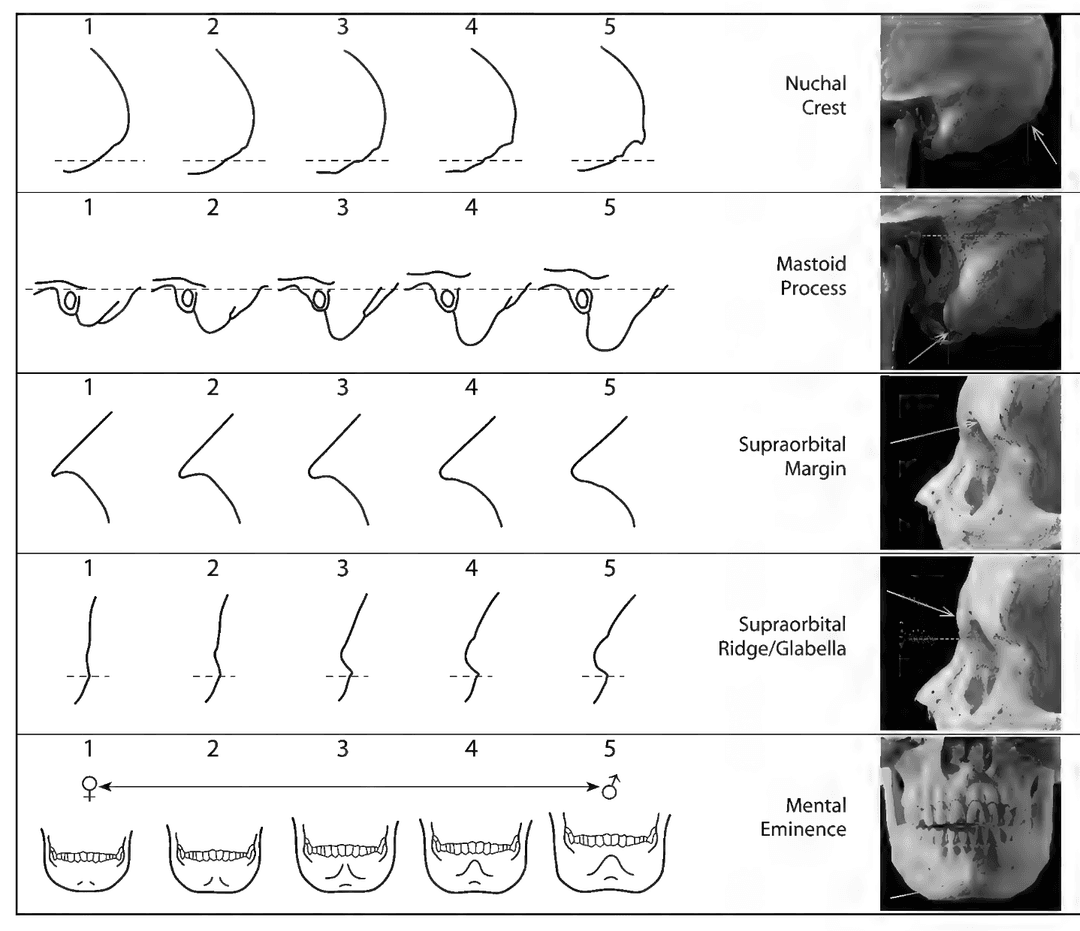
Men tend to have more robust facial muscles, affecting the bones at the skeletal-muscular sites (SMS).
Age Estimation
Subadult age estimation is based on stages of growth and development. Adult age estimation is based on stages of degeneration.
Phase systems are based on stages of development or degeneration. Component systems are based on individual features that can be observed and scored.
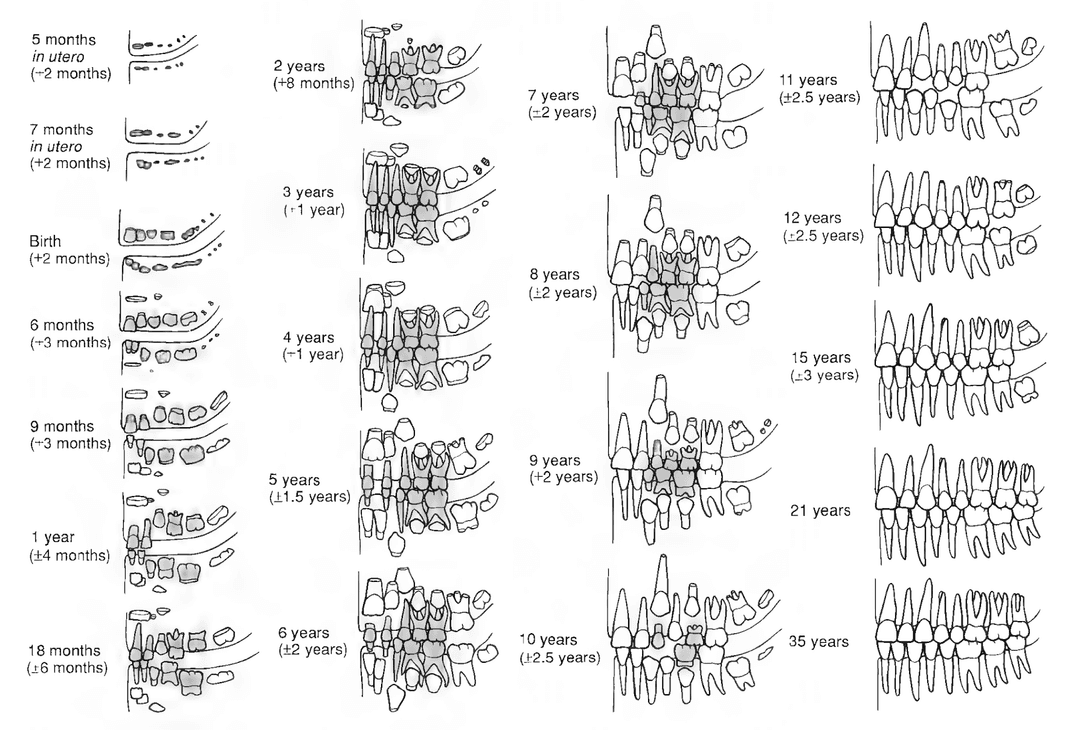
Subadult Age Estimation
Indicators:
- Dental development
- Appearance of ossification centers
- Suture closure (basilar and metopic)
- Long bone lengths
- Epiphyseal fusion
Malnourishment or ill health can stunt development. Dental development is the most reliable of all techniques.
Adult Age Estimation
Indicators:
- Pubic symphysis
- Auricular surface of the os coxae
- Cranial suture closure
- 4th sternal rib end
- Histology (secondary osteon counting)
The Todd system did age estimation based on the pubic symphysis. It has 10 phases.
The Suchey-Brooks system later modified the Todd system. It has 6 phases:
- Ridges and furrows, or billowing
- Billowing breaks down
- Bone builds up around joint margins
- The ventral rampart forms and the rim becomes more defined
- The porosity of the bone increases
- The rim breaks down

Lovejoy et al. made a phase system based on the auricular surface of the os coxae. It is not a very reliable method because two observers can easily disagree on the phase.
Lovejoy et al. made a component system based on the cranial suture closure. Younger individuals tend to have more open sutures, while older individuals tend to have more closed sutures. It is not a very reliable method because it is impacted by individual variation and environmental factors.
Transition analysis is a component system that uses observations throughout the skeleton. It uses Bayesian statistics to combine the skeletal observations with a prior age distribution. Traditional methods often underestimate the ages of older adults, partly because reference collections are biased.
Mortuary Archaeology
Mortuary archaeology is the study of the treatment of dead bodies in ancient societies.
Placement of the dead
- Cemeteries (Arlington)
- Pyramids
- Tzompantli
- Beneath the home
Body treatment
- Cinnabar (Tomb of the Red Queen)
- Mummification
- Embalming
- Cremation
Grave goods
- Pottery
- Food
Based on funerary treatment, we can make assumptions on socioeconomic status, role in life, and beliefs and traditions.
Bioarchaeology
Bioarchaeology is the application of biological anthropology (osteology) to the study of human remains recovered from archaeology sites. It is like forensic anthropology, but with a focus on the past.
Bioarchaeologists tend to ask demographic questions about
- Quality of life (health, diet, disease, growth and development)
- Behavior and lifestyle (occupational stress, habit-induced arthritis)
- Aesthetics and identity (tooth filing, dental inlays, avulsion, cranial modification)
- Warefare and violence (perimortem trauma)
- Population history (migration, ancestry)
Some analytic methods include:
- Life history (sex, age, ancestry estimation)
- Paleopathology
- Stable isotope analysis (for diet)
- Biodistance analysis
- Ancient DNA analysis
Linear enamel hypoplasia (LEH) is a line in the enamel that can be used to infer periods of stress during childhood.

Forensic Anthropology
Forensic anthropology is the study of the human skeleton in a medicolegal context.
Forensic anthropologists are needed in:
- Any context involving identification of a recently deceased human that has become a skeleton
- Death ocurring within 50 years
- Murder, abuse, and mass disaster
There are various other forensic experts in:
- Crime scene investigation
- Criminalistics
- Pathology (disease)
- Toxicology (poison)
- Odontology (teeth)
- Serology (bodily fluids)
- Radiology (imaging)
- Entomology (bugs)
- Geophysics
Forensic Archaeology
Forensic archaeology focuses on search, excavation and recovery, while forensic anthropology focses on analysis of those remains. This distinction exists in continental Europe, but not so much in the United States.
Contexts of body recovery:
- Buried
- Surface
- Mass fatalities (dismemberment, commingled)
- Fire scenes (complicated by multi-story)
- Oddities (cars, wells)
- Natural disasters (tsunamis, hurricanes, mudslides)
Surface search
- On the first pass, space people every few meters and walk the scene
- Put flags where there may be human remains
- Grid the scene and document it
- On the second pass, start at the flags and search outward
- Recover the skeletal remains
Clandestine grave search
- Dirt is dug up, body is placed in, and dirt is placed back in
- Graves tend to be bounded for 6-12 months before it settles
- Soil color and texture changes
- Plant growth changes
Laboratories
There are both coroners offices and medical examiners offices. A coroner is an elected official who signs off on cause of death, while a medical examiner is a MD who has expertise in forensic anthropology.
Sometimes forensic anthropologists are permanently on the payroll, while other times they are only brought in for dry bone cases.
A forensic anthropology cannot determine cause or manner of death; they can only make recommendations to the medical examiner. Cause of death is the reason for the loss of life (cancer, head trauma). Manner of death is the context of death (homicide, suicide, accidental, natural, unknown).
However, some forensic anthropologists are called in as expert witness in the courtroom to either defend the defense or prosecution. The Daubert guidelines govern the admissibility of evidence produced by expert witnesses.
To develop standards, forensic anthropologists use research collections with known sex, ancestry, pathologies, and cause of death. Reserach collections tend to be biased by ethnicity, class, and age.
Paleopathology
Paleopathology is the study of disease, nutritional deprivation, and mechanical stress in the past.
Disease
A disease is any conditional resulting in abnormality of the body or the mind. An infectious disease is a disease caused by a foreign pathogen.
Unfortunately, few diseases leave signatures of any kind on the human skeleton, and those that do may cause very similar skeletal reactions. It is common to list the most likely disease as well as alternatives. Additionally, there are not many well-documented skeletal samples that can be used for diagonsis.
Sources of infection:
- Bacterial (rarely)
- Viral (very rarely)
- Fungi (very rarely)
- Multicellular parasites (very rarely)
Examples of diseases that affect the skeleton include: treponematosis, tuberculosis, leprosy, blastomycosis, histoplasmosis, or cycsts made by larval taeworms.
At the cellular level, all bone disease are caused by either too much osteoblastic activity or osteoclastic activity.
New, irregular bone can grow on the periosteal surface, causing a periosteal reaction. This can be caused by trauma, localized infection, or systemic infection. This bone is called woven bone, since it doesn't integrate well with the original bone. Over time, it takes one a even denser appearance, called sclerotic bone. Sometimes the bone covers the blood vessels, causing vessel tracks to appear. Eventually, in well-healed bones, you will get mature, new bone, called striate bone. The tibia is the bone that is most commonly affected by periostosis.
Osteomyelitis is a bacterial infestation of bone. Its three characteristics are
- Involucrum (complete sheathing of old bone)
- Cloaca/fistula (opening for pus drainage)
- Sequestrum (isolated dead bone) Most can be attributed to Staphylococcus.
An individual's growth can be disrupted by disease, starvation, or trauma, causing the formation of Harris lines in the long bones.
Arthritis describes a condition that causes joint inflammation, pain, and stiffness. One common form of arthritis is degenerative joint disease (DJD) or osteoarthritis (OA). On the vertebrae, it can result in a slipped (herniatead) disc. On bone, it manifests as osteophytic lipping and eburnation.
Trauma and Fractures
There are four types of trauma:
- Blunt force
- Sharp force
- Projectile
- Miscellaneous
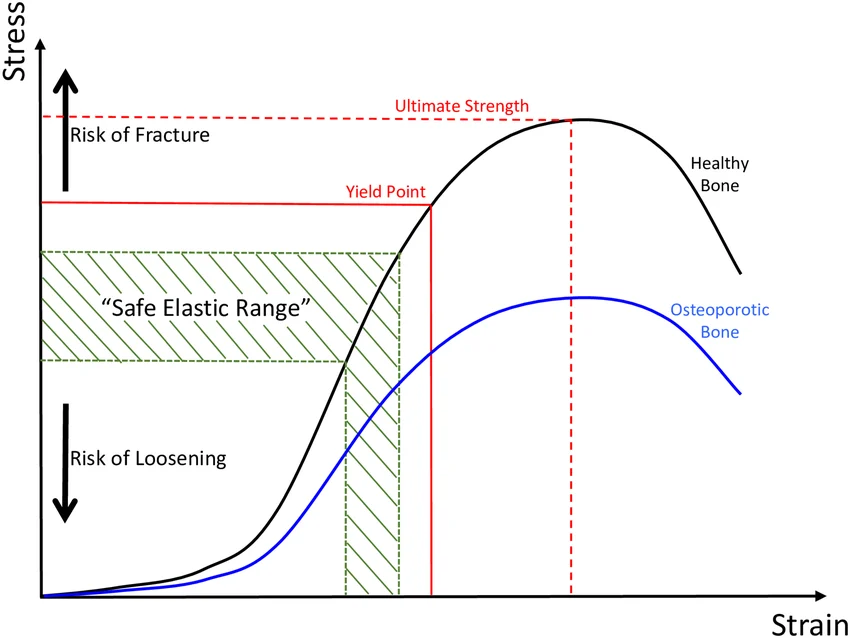
Bone can experience forces of compression, tension, bending, shear, and torsion.
Stress is force per unit area, while strain is deformation relative to original dimension. In the stress-strain curve, bone has an elastic region, a plastic region, and then a fracture region. In other words, living bones will allow some bending before fracturing.
Types of fractures
- A simple fracture is a complete separation of bone at the fracture site
- A greenstick fracture is an incomplete break, commonly occurring in children
- A comminuted fracture is a break of bone into multiple segments
- A axial compression fracture occurs when the bone collapses due to excessive pressure, often occurring in the vertebral column
- A Colles's fracture is a fracture of the wrist or distal radius
- A cranial fracture line (radiating or concentric) occur because of blunt force and ballistic trauma
Sharp force trauma can cause puncture, incision, cleft or notch, wastage.
Antemortem trauma contains evidence of some form of healing, such as porous/woven bone, rounded edges at fracture, or bone calluses.
References
- Human Osteology by Black, Folkens, and White
- Anatomy Standard